Contents
- Baby L
- Prosecution Opening Statement
- Defence Opening Statement
- Defence Closing Speech
- Agreed Facts
- Recorded Events and Messages (Babies L & M)
- NEW: Timeline Chart (Baby L)
- Lucy Letby in the Witness Box
- Direct Examination (Babies L & M)
- Cross-Examination
- NEW: Defence Closing Speech
- Witness Statements Agreed
- Family - Mother (Babies L & M)
- Family - Father (Babies L & M)
- Midwife (Babies L & M)
- Pharmacy Technician - Unnamed
- Witness Evidence
- Dr Sudeshna Bhowmik
- Neonatal Practitioner Amy Davies
- Dr Anthony Ukoh
- Dr A [Thirlwall: Dr U]
- Dr John Gibbs
- Dr Anna Milan
- Dr Gwen Wark
- Medical Expert Evidence
- Professor Peter Hindmarsh
- Police Interviews Summary
- NEW: Thirlwall Inquiry Evidence
Main Page
Baby L
Count 15: Attempted murder of Baby L on 9 April 2016. Alleged mechanism: Insulin Poisoning
Dr Shoo Lee's International Panel Summary Conclusions
BABY 12 SUMMARY [Baby L]
Baby 12 was a 33+2/7 week, 1.465 kg birth weight, twin 1, severe intrauterine growth
restricted (IUGR) preterm male infant, who was delivered by caesarean section for poor
growth and oligohydramnios at 1013 hours. On admission to the NICU, his initial blood
glucose was 1.9 and he was started on intravenous 10% dextrose at 100 ml/kg/day. The next
day, he was kept on intravenous TPN at 75 ml/kg/day plus 10% dextrose at 1 ml/kg/day plus
nasogastric feeds. His blood glucose was 3.6 at 0054 hours but dropped after that and was
low throughout the day (1.5 to 1.9). Blood tests showed c-peptide 264, Insulin 1079. At 1920
hours, his dextrose infusion was increased to 12.5% and blood glucose improved to 2.0 to
2.4. The next day, his blood glucose ranged from 2.1 to 2.4. The next day, a long line was
inserted and his dextrose infusion was increased to 15% at 0130 hours and fluid volume
increased at 0700 hours. His blood glucose stabilized after that from 2.7 to
3.0. Feeds were increased, the intravenous infusion was weaned off, and he was discharged
home.
CONVICTION
It was alleged that Baby 12 received exogenous insulin which caused hypoglycemia. The
evidence is based on a high insulin to low peptide level ratio (I/C ratio).
PANEL OPINION
It is common for preterm and IUGR infants to have hypoglycemia, due to their limited
glycogen and fat stores, inability to generate new glucose using gluconeogenesis pathways,
higher metabolic demands due to a relatively larger brain size, and inability to mount a
counter-regulatory response to hypoglycemia. Baby 12’s blood glucose dropped from 0054
hours on day after admission but his dextrose concentration was not increased until 1920
hours. This is a long interval without adequate sugar and intervention should have been
earlier. His blood sugar improved in response to 2.0 to 2.4. However, this is still low and
further intervention was necessary. Again, there was delay, and his glucose concentration
was not increased to 15% until the next day at 0130 hours and the volume was not increased
until 0700 hours. His blood sugars improved to normal range after that. The fact that his
blood sugar improved each time the glucose infusion increased indicates that the
hypoglycemia persisted because insufficient dextrose was given for this infant’s needs.
Chase et al reported that premature infants have different normative standards for insulin and cpeptide than adults. The Insulin:C-peptide (I/C) ratio does not prove exogenous insulin was administered because the C-peptide was not low for preterm infants (20-45 percentile), potassium levels were normal (insulin decreases potassium), antibodies can store insulin in the blood, glucose levels should be lower if exogenous insulin was used, the infant’s glycaemic profile was inconsistent with insulin administration but consistent with the delivered IV feeding profile, the I/C ratio was within the expected range for preterm infants, and the immunoassay test is unreliable because interference factors can give false positive insulin readings.
CONCLUSIONS
1. Hypoglycemia was due to preterm birth and severe IUGR; it’s medical management
was inadequate.
2. Baby F’s [sic] insulin level and I/C ratio do not prove that exogenous insulin was used, and
are within the norm for preterm infants. Preterm infants and those will illness have
different normative standards compared to healthy adults and older children.
Prosecution Opening Statement
BackgroundChild L was born in April 2016. It is the prosecution case Letby poisoned Child L, while also attacking Child M - the twin.
Child L's blood glucose level was noted to be low and he was treated with a dextrose infusion. His condition improved and he was stable by the day-time shift of April 9.
Incident
Letby came on duty that day at 7.30am.
By this time, the prosecution say, Letby was supposed only to be working day shifts because the consultants were concerned about the correlation between her presence and unexpected deaths and life-threatening episodes on the night-shifts.
In the hours that followed, Child L's glucose levels fell abnormally low. He was given additional doses of glucose, but they proved ineffective.
The answers to these levels were found after a lab sample sent to the Royal Liverpool Teaching Hospital laboratory came back with results some time later.
The results of the test were "grossly abnormal", but nothing was done about it as Child L had, by the time the results came back, returned to normal.
The reading was "at the very top of the scale" the equipment could measure, the court hears.
There was no correspondingly high level of C-peptide: it was within the normal range. The only explanation for this anomaly is that what was being measured was synthetic insulin, which had not been prescribed to Child L but was stored and readily available in the neonatal unit.
The court is shown an 'infusion therapy prescription sheet', a written record of the dextrose bag fed to Child L.
The bag was running from noon on April 8, when it had been set up an hour earlier by Letby and another nurse.
Prosecutor Nicholas Johnson KC: "We say Lucy Letby added insulin to that bag of dextrose. She did it deliberately to kill [Child L].
"She had failed to kill [Child F] so gave an increased dose."
Letby had been present for the birth of Child L. She cared for him on his first day and the prosecution say would have been aware of his mild hypoglycaemia.
Child L's blood sugar level remained "dangerously low" through the day.
At 4.30pm, a new infusion bag was required and this was being applied when Child L, the twin brother, was being taken ill.
Medical experts
The prosecution says medical expert evidence is this was a case of insulin poisoning, administered intravenously via Child L's liquid feed.
Police interviews
In police interview, Letby said she was aware of Child L's low blood sugar levels and knew the insulin was kept in a locked fridge, with a variety of other drugs. Keys were passed around nursing staff and there was no record of who held the keys at any time.
She agreed the insulin could not have been administered accidentally, but denied being responsible.
Her explanation was it must have been in one of the bags already being received.
The prosecution say that is not a credible possibility.
Defence Opening Statement
For Child F and Child L, the children allegedly poisoned with insulin, the defence "cannot say what has happened"."It is difficult to say if you don't know," Mr Myers said.
"So much has been said about these. These are not simple allegations which can automatically lead to a conviction."
The defence say Child E's TPN bag was put up by Letby in August 2015 and hours later there were blood sugar problems. That bag was replaced, in the absence of Letby, but the problems continued.
The sample taken came from "the second bag", the defence say.
A professor had given "three possible explanations", none of which identified Letby as a culprit.
For Child L, there were issues with the documentation provided, so those are challenged, the defence say.
There is "nothing to say" Letby was directly involved in the acts.
Defence Closing Speech
Mr Myers refers to the case of Child L. He says it is the second of the two insulin counts, where Child L had low blood sugar for a period of 53 hours, as identified by Professor Peter Hindmarsh. He says the laboratory result, if accurate, shows artificial insulin administered exgoneously.
Mr Myers says Letby was seeing friends, going on holiday, enjoying salsa, a win at the Grand National. He says it is important to keep in mind the person who these allegations are aimed at. He says at this time, her main concern was moving house "and this was on her mind". Text messages are shown to the court showing conversations with Letby about her new home in Chester, having been at hospital residence.
Mr Myers says it is important to consider each count separately. He says it is not accepted Letby has committed this offence. He says there was a delay in getting the sample taken from Child L sorted, and was outside the 30-minute guidance, whether it was taken at noon or 3.45pm. He says the Countess of Chester Hospital Pathology department records the lab specimen report notes it was received at 6.26pm. He says Dr Anthony Ukoh says the sample was taken at noon.
Mr Myers says nurse Mary Griffiths had said there was a delay in podding the blood sample due to what happened with Child M. He says it is a "point of contention" that the delay in processing the sample is "one thing to keep in mind" when processing the results. He says apart from the "apparently" low blood sugar level, there was no ill effect observed on Child L, which he says is "extraordinary". He asks how that is evidence of poisoning. He says the blood sugar level reading in the sample, was 2.8, a "relatively healthy reading". would be inconsistent with the insulin and insulin c-peptide. Professor Hindmarsh said it was a plasma reading, so would give a different blood sugar level reading than a heel prick, and it was said it would be more like '2.4'. He says the heel prick tests showed a blood sugar level reading of 1.6 at noon. The ones at 3pm and 4pm are 1.5. He says it does raise a question on the accuracy of the blood sugar readings.
The trial is resuming after a short break.
Mr Myers says there was one detail he had omitted before the break. He says at 3.40pm, bolus of 10% dextrose was administered for Child L. He says the prosecution says that would account for the higher blood glucose reading. He says the problem of a 1.5 [heel prick] reading at 4pm still remains, as does the 3pm 1.5 reading. He says it is difficult to work out what effect it would have.
He says Letby cannot have interfered with the bags in the way it is alleged. He says the bags are changed during the 53 hours Child L was recorded to have low blood sugar readings, during which five bags were used. He says a number of bag changes took place for which Letby was not involved in. He says the prosecution alleged Letby was 'setting up an issue' of hypoglycaemia for Child L. He says it does not follow as Child L would be a focus on blood sugar levels, and someone with harmful intent would not identify an issue that was going to be detected anyway. He says Letby would be drawing attention to it. He says Child L's designated nurse was recorded on the neonatal schedule as being a co-signer for 9.25am-9.29am prescriptions. He says that is when the electronic prescriptions are inputted. He says Dr Ukoh would also be in room 1 that morning (where Child L and Child M are) as part of his ward round. He says there is no record of him outside of room 1 during the time Letby was alleged by the prosecution to administer insulin in Child L [about 9.30am].
Mr Myers says the theory Letby spiked the various bags with insulin is "contrived and arfiticial", and the mechanics of it are "unrealistic". He asks how Letby could predict to add insulin to the dextrose bags in storage, which would be used for all babies on the unit, only for Child L. He says the theory of 'sticky insulin' is "mixed". He says there is a lot of bag changes over 56 hours. Prof Hindmarsh was cross-examined about it, if the 'sticky insulin' would run out at some point. He said it would. He said over time, additional insulin would be required to maintain the levels [of low blood sugar levels].
Mr Myers says whatever the reason for Letby accumulating paperwork [at home] in the case of Child L, it does not provide sufficient evidence of an intent to harm the baby.
Mr Myers says Letby subsequently cared for Child L after April 9-11, and it is "utterly inconsistent" with someone wanting to target that child to harm or kill them.
Agreed Facts
Recorded Events and Messages (Babies L & M)
8th April 2016:
Intelligence analyst is talking the court through the sequence
of events for Child L and Child M, twin boys born on April 8.
10.30-10.59am: Child L was admitted to the neonatal unit at 10.30am, and had observations taken by Lucy Letby, with a blood sugar reading of 1.9 recorded at 10.58am. He was treated with a 10% dextrose (sugar) infusion.
Lucy Letby's note, written in retrospect at 5.42pm, noted the blood sugar reading of 1.9, with the registrar commencing dextrose and expressed breast milk.
At 12.14pm, the blood sugar reading had risen to 2.5.
Lucy Letby records communication with Child L and Child M's parents: "Parents were shown babies in theatre and had a quick cuddle....Photographs given and visiting hours discussed. Daddy visited the unit and had cuddles."
4pm: For Child L, a blood sugar reading of 5.8 is recorded at 4pm.
Letby records for Child L at birth "Initially had some recession with a raised respiratory rate, quickly normalised and remained self ventilating in air. Blood gases good... "2 Hourly feeds, NG/bottle. Minimal aspirates obtained..." Recording communication with the parents: "Parents updated by myself on CLS and photograph taken....fully updated on care by myself and reg Bhowmik. Aware of need for septic screen..."
A 6pm blood gas reading records blood sugar of 3.3
6.15pm: Letby messages a colleague at 6.15pm - "Unpacking! Stuff everywhere lol! May do an extra shift this weekend x" The court previously heard Letby had recently moved into a home near the hospital. Letby messages her mother: "Think Im going to do tomorrow [Saturday, April 9] as an extra but go in a bit later."
9pm: Child L's blood sugar reading at 9pm is 2.3.
Letby's colleague Sophie Ellis messages her: "How's the house pal?
Xxx"
Letby: "Hey, it feels a bit weird having a whole house but it's good thanks, although
stuff everywhere as moved in properly on Tue and been at work Wed, Thurs and today...",
followed by a monkey emoji with its hands over its eyes.
Sophie Ellis: "...it'll feel more homely once you've sorted everything out." She also
asks about how busy the unit is.
Letby: "...Unit is busy, no-one particularly unwell just volume and few people off sick.
I prefer 4 days to 4 nights..." Letby adds: 'We've got nice mix of babies at the mo really.
Shift goes quick anyway!'
10pm-Midnight: Child L's blood sugar reading is 2.2 at 10pm, then 3.6 at midnight.
Further medications are administered throughout the night. Agency nurse Tracey Jones records notes for Child L from the night shift, noting the cannula was knocked out by the baby boy during the night so was reinserted. There had been no contact with the parents during the night.
9th April 2016:
For the day shift on April 9, 2016, Lucy Letby is a designated nurse
for two babies in nursery 1. Mary Griffith is the designated nurse for Child L and Child M,
who are the other two babies in room 1. Four babies are in room 2, three in room 3 and four
in room 4. There are seven designated nurses for the neonatal unit babies in total.
10am: Child L records a blood sugar reading of 1.9 at 10am, pre-feed. Nurse Mary Griffith records notes, written retrospectively, saying the IV dextrose [infusion] was increased for Child L.
10.34am: Letby messages colleague Ailsa Simpson at 10.34am, wishing her good luck at picking the horses at the Grand National that day, and that her feet don't get too sore.
11am: Child L's blood sugar reading is 1.6 at 11am.
12pm: A handwritten entry for hypo screen results at noon, not attributed to a name, record results for Child L. Child L's blood sugar reading is 1.6 at noon, pre-feed. Letby co-signs a 10% dextrose infusion for Child L, around noon.
12.30pm: Notes for Child M record that designated nurse Mary Griffith took a break around 12.30pm.
Letby is engaged in messaging people between 11.12am and 12.33pm. Letby messages Ailsa Simpson shortly afterwards: "Oh good hope you have a fab time. Im in work doing an extra! x" Letby also messages her mother, asking if her father was betting on the Grand National, and if so, to put a bet on grey horses for her. Her mother replies that has already been done.
The court hears Letby continues to be involved in messaging, including a group message to colleagues and friends: "Sorry guys mad 4 busy days in work..." then invites the three people to crash at hers, apologising she hasn't fully unpacked yet. She adds: "Got magnum prosecco and vodka woop. No disco ball but sure we can manage. x"
2pm-3.40pm: Child L's blood sugar reading is recorded as 2.0 at 2pm, and 1.5 at 3pm. Letby is a co-signer for the administration of medication at 3.35pm. Mary Griffith records a blood sample was taken from Child L at this time, which was taken to the Royal Liverpool Teaching Hospital for analysis. The prosecution say the blood sample had a very high insulin level recorded, and a low level of C-peptide. Child L was also given a bolus of dextrose, prescribed at 3.35pm and administered at 3.40pm.
A note from the hospital's pathology department records the blood specimen sample for Child L. The blood was "taken for lab but due to emergency not poded at once", nurse Mary Griffith records. That one emergency identified in the neonatal unit, the prosecution tells the court, was for the twin brother, Child M's "dramatic collapse".
4pm: Child L's blood sugar reading at 4pm is 1.5.
Child M's collapse is recorded at this time. A crash call is put out. Friends message Lucy Letby around this time, saying they can have "an unpacking party". For Child L, the dextrose administration is increased to 12.5%, from 10%.
5pm: Child L's blood sugar reading at 5pm is 1.7, which was "still very low", the prosecution say.
5.28pm: Letby's mother messages Letby at 5.28pm telling her: "You've won rule the world :-D xxx"
6pm: Child L's blood sugar reading at 6pm is 1.9.
Letby responds to a colleague at 6.01pm: "Haha why not!! Work has been s***e but...I have just won £135 on Grand National!!" She also sent a group message: "Unpacking party sounds good to me with the flavoured vodka...Just won the Grand National!"
The pathology records the lab specimen of a blood sample for Child L. Among the blood test results sought for the sample are insulin and C-peptide. The insulin level is recorded as 1,099, and the C-peptide is recorded as 264. These readings are entered into the system on April 14, having obtained the results from Liverpool. The C-peptide "should be 5-10 times the level of insulin", but the ratio is recorded as 0.2.
Child L is recorded to have hypoglycaemia [low blood sugar]. Doctors record the hypoglycaemia continued despite the regular infusions of dextrose throughout the day.
8pm: Child L has a blood sugar reading of 2.0 at 8pm.
9pm: Child L's blood sugar at 9pm is 2.4. Letby records notes for Child M at 9.22pm.
10pm: Child L's blood sugar reading at 10pm is 2.3.
10.11pm: A colleague of Letby,
Belinda Simcock, messages her at 10.11pm: "Thanks for listening, I'm ok x"
Letby: "Don't need to thank me, glad you felt able to tell me..."
10th April 2016:
Midnight-2am: Child L's blood sugar
reading at midnight is 2.1, and remains "low" at 2.1 at 2am. A long line is inserted, with
an x-ray taken, and medication administered.
4am-7am: The blood sugar reading at 4am is 2.3, and 2.2 at 6am. The glucose is further increased, but the blood sugar reading "remains stubbornly low" at 2.2 at 7am.
9am-7am: It remains at 2.2 at 9am.
Letby receives a message from Yvonne Farmer asking if she wanted to do more overtime shifts on Sunday night, Monday day or Monday night, appreciating she may be tired, with Letby responding: "Sorry but need some days off now." She adds she could be on call for nights, and would be free for Thursday day/night shifts.
2pm: Child L's blood sugar reading at 2pm on Sunday had "normalised" at 3.0.
Letby refers to her previous shifts as "not nice" in a message to Jennifer Jones-Key. Jennifer Jones-Key says Letby 'hasn't got many nights' coming up on the rota, adding she likely won't see Letby as she works mainly nights herself. "We never see each other if we do work together as always mad shifts".
Afternoon: Child L was still receiving 15% dextrose through the afternoon of Sunday [10th April]. A nursing note made by Laura Eagles that afternoon records: "Blood sugars maintained...remains on 15% dextrose via long line...very unsettled at times." The family had been kept updated of the situation, according to a family communication note.
5pm: Child L's blood sugar levels were "normal" at 2.8 at 5pm. Samantha O'Brien becomes the designated nurse that night for Child L, and the 15% dextrose administration continues through the night.
9pm-2am: The blood sugar levels are 2.7 at 9pm, 2.9 at 11pm, 2.7 at 2am.
11th April 2016:
Samantha O'Brien, in
her nursing note, records: "...1% glucose infusing via long line in left leg,. 3 hourly
blood sugars, all have been above 2.6 so far this shift. Plan to continue [current
medication administration]... "Baby unsettled at times, settles with comfort measures."
5am: The blood sugar level is 2.9 at 5am on Monday, April 11.
8.45am: Letby messages a colleague at 8.45am, saying: "The unit is in dire way with staff," highlighting which trained staff were on duty and who else was on in the last shift, and who was off at that time. A colleague replies, in her message: "that's terrible" Letby replies the overall situation was "not good", "mad and poor skill mix".
11am: Child L's blood sugar readings are 2.8 at 11am. Dr Huw Mayberry, in a clinical note, records the feeds/fluids for Child L, which were increased due to low blood sugar and falling sodium levels.
3pm-5pm: Child L's blood sugar at 3pm is 3.5, remaining at 3.5 at 5pm. Nurse Belinda Simcock said registrar Mayberry was aware of the 3.5 readings, and if they continued to remain above three, then feeds would be increased.
7pm: The blood sugar increases to 4.7 at 7pm.
3rd May 2016:
Child L continued to be cared for at the hospital's neonatal unit
until May 3, and was then discharged.
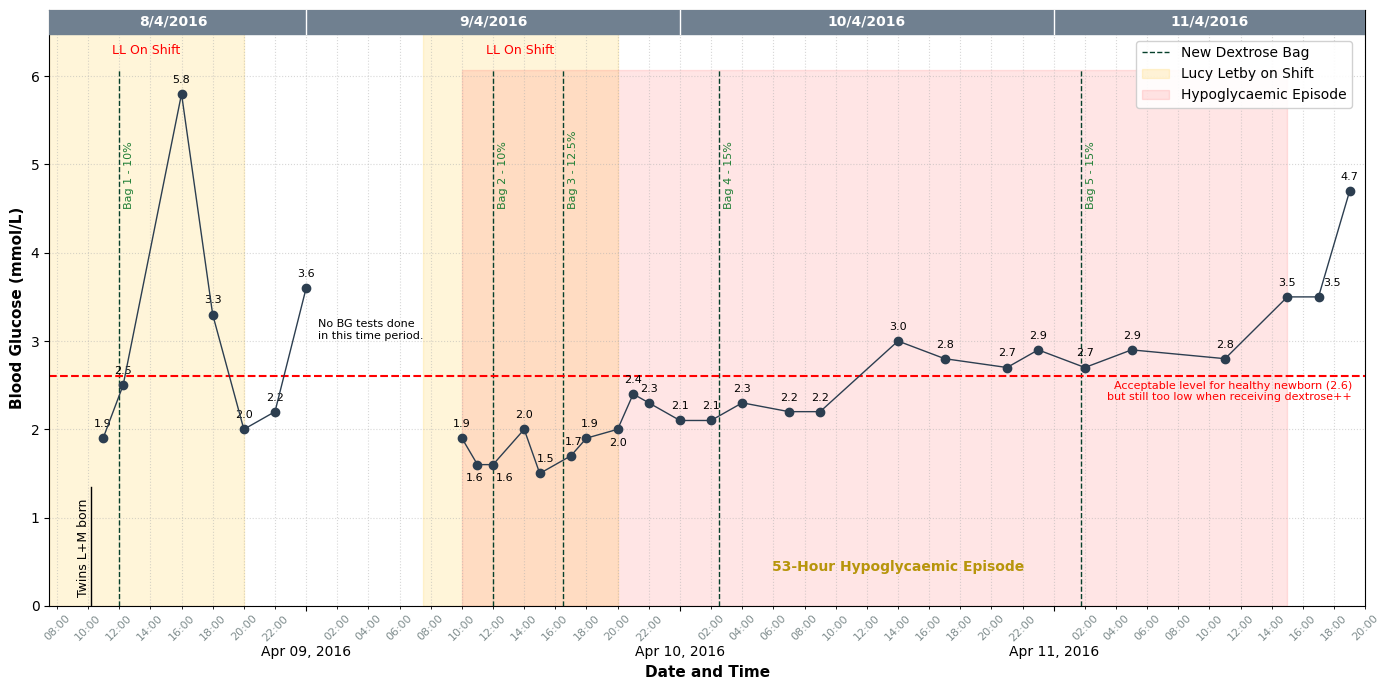
Baby L: Timeline of Blood Glucose Readings and Dextrose Infusions
Lucy Letby in the Witness Box
Direct Examination (Babies L & M)
Lucy Letby gave this evidence on 16th May 2023.Mr Myers moves on to the cases of twins, Child L and Child M, born on April 8, 2016 at 33 weeks and 2 days gestation. Letby confirms she is still working and caring for babies, working a mixture of day and night shifts, at the hospital, during this time. She says, in reply to what her intentions were for the babies: "To provide the best care possible." She estimates she had cared for about "100" babies during these few months.
Child L was born weighing 1,465g. Child L later struggled with low blood sugar. A blood sample was taken for Child L - the insulin level read 1,099, insulin C-Peptide 264. The insulin was "far higher" than the C-peptide reading, indicating, Mr Myers, insulin had been administered to Child L. Child M weighed 1,705g. Child M later had a desaturation, which it is alleged Letby had caused.
On April 8, Sophie Ellis messaged Letby: "How's the house pal? Xxx"
Letby responds: "Hey, it's feels a bit weird having a whole house but It's good
thanks, although stuff everywhere as moved in properly on Tue & been at work Wed Thurs &
today ?. Doing tomorrow as an extra so I'll see you tomorrow night. Won't be such an early
start for you now back in Chester!..."
The reply: "Yeah I bet it does, it'll feel more homely once you've sorted everything
out. Jeeeez 4 [Long Day shifts] in a row, are you ok?! ? I know yay and I don't have to
pay for petrol, it's cost me a fortune ?゚リᄅ. Yeah they are ? haven't seen them for a
while. What's the unit like? Xxx"
Letby: "Yeah I'll get there in time. Petrol & tunnel soon mounts up doesn't it! Can
you claim travel expenses? I couldn't for 405. Unit is busy, No one particularly unwell
just volume & few people off sick. I prefer 4 days to 4 nights. Least tomorrow is an extra
& Sat pay! ?. Awe that'll be nice hope weather a bit better for you! X"
SE: "Yeah we can. Omg really, how come? That's 7 weeks as well isn't it? Yeah, 4
nights are awful. Ah that's not too bad then. Think I'd prefer to keep busy. I think it's
meant to rain...dammit xxx"
LL: "Eirian said something about the induction being paid for by the trust whereas the
405 comes out of network budget so won't pay as its an expected part of role to progress
etc. Mad really & costs a bomb! We've got nice mix of babies at the mo really. Shift goes
quick anyway! Grr typical April showers haha. [Colleague] is in Thailand & It's been
44degrees today! X" Letby said it was a "massive" life moment for her to move into her new
house, and her main focus was on "sorting out the house". Letby says the unit was "still
fairly busy" at this point.
On April 11, Letby messages a colleague: "The unit is in dire way with staff..." She says the unit had 'banker agency staff' and band 5s who did not have the ITU course. She says the unit being busy was "often discussed by staff".
Letby recalls being involved with the care of the twin boys, and looked after one of the twins in the transfer to the neonatal unit. The twins were placed in nursery room 1, and Letby cared for Child L that first day.
The following day, April 9, Child M was in a different place in room 1, following admission of other babies overnight. Child L and Child M were in adjacent beds in room 1, the court hears.
Letby tells the court a baby's blood sugar levels are checked "within the first hour of life". Child L's first blood sugar reading is "low" - 1.9. The baby would be offered "a milk feed" via a bottle or NG tube, and the blood sugar would be checked after another hour. This did not happen with Child L, and he was administered 10% dextrose [sugar infusion], which Letby says was outside the guidelines, a decision made by Dr Bhowmik. Letby's notes: 'Advised by Dr Bhowmik to commence 10% glucose...' Letby added in the notes that she and the shift leader advised this deviated from the usual policies.
A glucose bag was hung up for Child L. Letby said she cannot recall who hung up the bag - she said it would either have been herself or nurse Amy Davies. Child L had normal blood sugar levels the rest of the day. She tells the court she would have ended her shift at about 8pm.
Mr Myers says for April 9, 2016, there are no recordings of blood sugar for 3am, 4am or 5am. A 10am reading of 1.9 is "too low". It is 1.6 at noon. 2pm it is 2. Letby had come on duty at 7.30am. The infusion rate has been changed at noon. A 10% dextrose bolus is administered at 3.40pm. Letby says she cannot recall who was involved in that administration. At 4pm, the blood sugar level is 1.5. At 4.30pm, a 12.5% dextrose bag is administered by two nurses including Ashleigh Hudson. The readings remain "low" up to midnight. On April 10, at 2am, the reading is 2.1, then a new 15% glucose bag is administered. 4am it is 2.3, 6am 2.2, at 2pm it is 3 - "an adequate level", but then drops for the rest of the day. A 15% glucose bag's rate is changed early on April 11, and a new bag is administered that day. The readings are 2.7, 2.9, 2.8 throughout that morning. At 3pm it is 3.5, and blood sugar is said to have stabilised.
The trial is resuming following its lunch break. Benjamin Myers KC is continuing to ask Lucy Letby questions in the cases of twins Child L and Child M. The infusion therapy prescription sheet is shown for Child L, with prescriptions for April 8-9. The first entry is for April 8, 11am, for a 500ml, 10% dextrose infusion, via the IV line. Dr Bhowmik authorised the prescription and the bag additive. Lucy Letby and Amy Davies set up the infusion. The first two infusion prescriptions have a line through them as, Lucy Letby explains, the rate of infusion was changed twice. It went from 4.2ml/hr to 3.6ml/hr to 4.4ml/hr. The 4.4ml/hr rate was started, using the same bag, at noon. The bags were stored in a cupboard in room 1. This was in a separate room from the insulin bags in a cupboard in a corridor.
Mr Myers asks how commonly dextrose is used on the unit. Letby says "very commonly", adding that a 10% dextrose solution would be administered 'all the time'. They would be used "for generic use".
Letby sent a message to her mother on April 8: "Think Im going to do tomorrow as an extra but Go in a bit later. Extra money and Sat pay xX" This was to be Letby's fourth long day shift in a row (April 6-9), the maximum normally allowed for Countess staff at the unit, the court hears. For the April 9 long day, Letby was designated nurse for two babies in room 1, and Mary Griffith was designated nurse for Child L and Child M, also in room 1.
Child L's 10% dextrose bag was changed on April 9 to a new 10%
dextrose bag, at noon, signed by Letby and Mary Griffith. That bag "would have come from
the generic bags in room 1", Letby says. She does not recall who would have put it up for
Child L. The equipment involved in setting it up would come from nursery room 1. Mr Myers
says prior to this, Child L had a blood glucose reading of 1.9 at 10am. Letby says the
initial infusion bag would still have been in place at this time. She says she cannot
explain why that reading was low, and did not do anything to cause that low blood sugar
reading. She adds she did not do anything to cause the later recorded insulin levels to be
high for Child L.
Mr Myers: "Had you done anything to affect insulin?"
Letby: "No." Letby says as well as herself and Mary Griffith being the two designated
nurses in that day, there were other nurses 'coming and going' in room 1, along with
parents "present throughout the day".
Nursing notes for one of Letby's designated babies - a high-dependency baby - are shown to the court. They include: 'Parents visiting carrying out feeds and cares....At 1600 parents were asked to leave the nursery due to a sick baby needing treatment, parents were understanding of this and left for the evening.' Letby says this was when Child M had deteriorated. She said this would be "common practice" to ask parents to leave in such an event. Letby adds the visiting times were 24 hours and parents would visit throughout the day.
Nursing notes by Mary Griffith record, for Child M on April 9: '...at 12.15 noted that his stomach was a little distended and his work of breathing was increased. Was then sent for my break and [colleague] did the 12.30 feed...had an aspirate of 5mls...temp returned to normal and baby settled.
At 1600 baby went apnoeic and had a profound brady and desat. Full resus commenced at 1602...care handed over to SN L Letby.' Letby tells the court Mary Griffith was, at this point, not trained for the type of intensive care Child M required, which was why care was handed over to her.
A prescription chart shows Lucy Letby is involved, with Mary Griffith, in the administration of antibiotics for Child M at 3.45pm. Letby says the line would also be 'flushed' after this is administrated. Letby says at the time of Child M's deterioration, Child L was requiring further dextrose. A chart shows Letby was involved in administering a 4.3ml, 10% dextrose bolus at 3.35pm, administered at 3.40pm. A 12.5% dextrose infusion is made up by nursing staff "in response to ongoing low blood sugars", which begins at 3.35pm and the infusion starts at 4.30pm. The infusion start is administered by Belinda Simcock and Ashleigh Hudson. Letby says she and Mary Griffith had been "preparing a bag" for Child L. She says Mary Griffith was the "sterile nurse" and Letby was assisting her between 3.45pm and 4pm.
Asked when she first became aware of a problem, Letby said the alarm went off and Child M was "not breathing" and "clearly struggling". Mary Griffith and another nurse were in there. Letby recalls asking parents to leave. Letby says she began initiating Neopuff "straight away", but because it didn't reach, the face mask fell on the floor, and Letby asked for another face mask for Child M. She adds she and Mary Griffith "abandoned" the making up of the bag, and "the focus was on [Child M]". Two other nurses 'started the procedure from the beginning' [of making up a new dextrose bag for Child L]. Letby said that would be "standard practice", to make sure staff were sure the new bag had the correct, required concentrations.
Letby, asked again by Mr Myers, denies doing anything to affect Child L's insulin levels. She agrees Child L's blood sugar levels remained low, and cannot explain why that was the case.
Letby says another nurse and Dr Ravi Jayaram came to assist Child M. She says she cannot recall any observation or discussion of discolouration on Child M's skin.
Letby says she left later than 8pm that night as she had a lot of documentation to file at the end of her shift. A nursing note for Child M by Letby is recorded as being written between 9.14pm-9.22pm on April 9. Letby said this was after attending to the clinical needs of Child M. Letby said she would write contemporaneous notes on the back of handover sheets or on paper towels to keep track during the day.
The court is shown a few notes written on paper towels which were recovered from 'the Morrisons bag' at Letby's home by police. There are also medical notes on sheets of paper. They feature notes in the resuscitation of Child M. Letby says the notes were kept in the pocket of her uniform, and came home in her uniform. She says she did not have any other use for them. Also among the notes is a blood gas printout for Child M. Asked to explain that note, Letby says she had put it in her pocket and taken it home. Asked by Mr Myers why she hadn't binned it: "That is an error on my part." She denies having any use for the notes.
Letby confirms she continued to care "quite frequently" for Child L and Child M following their events, until they were both discharged from hospital on May 3. Nursing and family communication notes by Letby in respect of Child L and Child M are shown to the court on April 16, 17, 24, 25, including when Letby had been their designated nurse. "I did my best for them," Letby tells the court.
Cross-Examination
Lucy Letby gave this evidence on 5th June 2023.Mr Johnson moves to the second insulin case, for Child L, who was a twin to Child M. Letby's defence statement said she had done nothing wrong and had not deliberately harmed either twin. Letby agrees this was a case when she challenged doctors if she believed the course of care being given was not correct. Letby said in her defence statement the unit was "exceptionally busy" on April 9, 2016, the day after Child L and Child M had been born. Letby said, at the time, she "could not understand" Child L's insulin levels at the time and "could not understand" why there was not an investigation at the time.
Letby denies 'using' the hypoglycaemic pathway not being followed as an 'opportunity' to attack Child L.
Letby says she accepts someone put insulin into the dextrose solution for Child L, and accepts there would be "no reason" for doing this, and that it would be "highly dangerous".
Letby accepts the blood results 'prove' insulin was placed in the
dextrose solution. Prof Hindmarsh had previously given evidence to say insulin had been
administered between midnight and 9.30am on April 9.
NJ: "Do you accept that?"
LL: "Yes."
Mr Johnson says the insulin administered to Child L was a 'targeted
attack' as the dextrose bag had been in place since noon on April 8. "It follows that
insulin was administered while the [dextrose] bag was hanging, doesn't it?"
Letby: "I don't know." Mr Johnson talks through the process and repeats that, from
evidence, the bag must have been in place when insulin was administered.
LL: "If that's what the expert suggests, yes."
NJ: "It follows that it was a targeted attack?"
LL: "I can't answer that."
Mr Johnson says the only two staff members on duty for both days, when Child F and Child L were poisoned with insulin, were Letby and Belinda Williamson [Simcock]. A staffing rota for the April 9 day shift is shown to the court. Child L and Child M are in room 1, with designated nurse Mary Griffith. Letby is designated nurse for two other babies in room 1. Belinda Williamson is the designated nurse for three babies in room 3. Four babies are in room 2 and four babies are in room 4.
The neonatal schedule for April 9 is shown. Mr Johnson says it is to
show what Lucy Letby was doing between 9am-9.30am. The schedule shows Letby was a
co-signer for medication for one baby in room 2, and giving a feed to her designated baby
in room 1. Letby was the co-signer for medication for a room 1 designated baby around
9.10am. Mr Johnson says a series of prescriptions for three different babies at
9.25-9.29am, co-signed by a nursery nurse and Mary Griffith, gave Letby the "opportunity"
to administer the insulin for Child L. Letby says: "No, I don't know how the insulin got
there." Mr Johnson says it has already been established the insulin was administered on
the unit, on the bag that was connected to Child L throughout that time.
NJ: "That's what it's a targeted attack, isn't it?"
Letby pauses.
NJ: "What do you say?"
LL: "Not by me it wasn't." Letby says she can "only answer for herself" in relation to
the accusation by Mr Johnson that the insulin poisoning for Child F and Child L "can only
be you or Belinda Simcock".
Mr Johnson says despite the fact the bag was changed at noon on
April 9, the insulin kept being administered to Child L, "didn't it?"
Letby: "Yes."
Mr Johnson says "we know that" because the blood sample taken to the lab
was taken at 3.45pm "contained exogenous insulin".
Letby: "I can't recall."
Mr Johnson says Child L was targeted with a second bag of
insulin.
Letby: "I'd have to be guided by the evidence - the expert evidence."
Mr Johnson says
a third bag is hung up at 4.30pm. The hypoglycaemia "continued".
Letby agrees.
The fourth bag, hung up the following day "when you [Letby] were not working"
was put up, and the hypoglycaemia "gradually resolved".
Letby agrees.
Mr Johnson says the reason for the hypoglycaemia was that someone
had poisoned Child L through 'at least two' bags of insulin.
LL: "Yes."
NJ: "And that was you, wasn't it?"
LL: "No."
Witness Statements Agreed (Babies L & M)
Family - Mother (Babies L & M)
The court is now hearing a statement from the mother of Child L and Child M, who had had a "routine Pregnancy" until a stage when she was "not well".She recalls being "surprised and shocked" at being told she had to be admitted to hospital.
She stayed there for 15-17 days and was asked if she was going to deliver naturally or via a C-section. Staff had looked through her file and were "worried", so the decision was made for the birth to take place, via c-section, on April 8.
The babies, weighing 3lb each, looked "very nice".
The family were taken to the neonatal unit to see them in room 1 the following day and the family were "happy", and at that time it was not known what they were going to be called - deciding on the names a week later.
Later, the mother was asked by a nurse named Yvonne to come down as soon as possible. She came down and saw Child M had collapsed and chest compressions were under way.
She was praying to see her, asking God to see them. Child L was ok on the other side of the room, and Lucy Letby was present.
She said her mind was "totally blank" and she just prayed.
After what felt like "hours", Child M had stabilised.
Each day, the mother would come down daily to see the twins, who had stabilised.
Three weeks later, the mother was discharged, and she continued to visit daily until the twin boys were discharged. They hadn't put much weight on and were small, but otherwise healthy.
Child M had "no after effects for what happened to him".
Family - Father (Babies L & M)
A statement from the father is now being read out. He said he was "shocked" at the news his wife needed to go to hospital due to concerns over the pregnancy, and she stayed there for "over two weeks" before the C-section birth took place.The doctor said the babies looked "very healthy" before being taken to the neonatal unit by Lucy Letby and another nurse.
He saw the twins a couple of hours later and they were "both still fine".
The following day, the family visited - "we were both proud parents, and very happy".
Within 10 minutes of being on the ward, the father "rushed" back to the neonatal unit, where he saw a doctor doing chest compressions on Child M.
He said: "It was a very distressing image, and one that still is in my mind."
The staff said they didn't know what had happened to Child M, and Child M had had a heart attack.
Child M later stabilised after about half an hour, and there were no further issues with the twins in subsequent care.
Child M had a brain scan, with 'no damage' recorded.
The twins were "only on the unit because they didn't weigh enough", and it was "a relief to get the boys home".
Midwife (Babies L & M)
A statement from the midwife is now being read out to the court.She said there was concern one of the twins was not growing as he should have in the womb, so an elective surgery took place so there were no further complications with the lack of growth.
Both babies "were in good condition" and there was time for "a quick cuddle" with the parents before the twins were taken to the neonatal unit "without any problems".
Both twins began crying after birth, one of them requiring a little extra help to do so.
The 'Apgar score', which records the conditions of the babies shortly after birth, recorded 10/10 scores for both twins at 10 minutes after birth.
Child M has a low oxygen saturation rate, but he had that rectified with breathing support.
Pharmacy Technician - Unnamed
From Dan O’Donohue Twitter (20/02/2023)Court has just been read a statement from a pharmacy technician who has worked at the Countess of Chester since 1991. A review of her records show that in 2014, three vials of insulin were ordered to the neonatal unit, six in 2015 and two in 2016
Witness Evidence
Dr Sudeshna Bhowmik
See also: INQ0102352 – Witness Statement of Dr Sudeshna Bhowmik, dated 20/06/2024
Dr Sudeshna Bhowmik, who was working as a paediatric trainee at the time in April 2016 at the Countess of Chester Hospital, has been called to give evidence.She says, outside of the clinical notes, she has no memory of the twins, Child L and Child M.
She confirms, from the notes, she was present at the birth of the twins, citing an IV line for Child L on April 8 at 11.15am, which was "quite a routine procedure to be done on the neonatal unit".
The baby was "generally well", although the breathing rate was "a little elevated".
The court hears that was not a concern as that would usually be the case for babies born via C-section.
The weight of 1.465kg [3lb 3oz] was "quite low", and the blood sugar of 1.9 was "a little bit low", which can be found in premature babies who are quite small.
With glucose feeds, that would "stabilise".
The plan was to commence dextrose via IV fluids and feeds via expressed breast milk, to see if the latter would be tolerated 'in small amounts'.
She added at that time, there was no need to administer antibiotics. Dr Bhowmik tells the court with Child M showing signs of jaundice, however, that plan may need to have been revisited.
The plan was also to repeat the blood sugars in half an hour.
She says most pre-term babies will have IV fluids, and this was altered for Child L because of the baby boy's weight and glucose levels.
Cross Examination
Benjamin Myers KC, for Letby's defence, asks Dr Bhowmik to clarify the blood sugar readings for a healthy baby. 2.6 and above is healthy.
Mr Myers says Child L was recorded as having a 1.9 reading a couple of hours after birth.
He asks Dr Bhowmik questions about a 'hypoglycaemic pathway'. Dr Bhowmik says the correct course at the time would have been to start treating hypoglycaemia at the neonatal unit via IV fluids.
She tells the court she does not recall when the bag of IV fluids was put up, or who administered that bag.
An infusion chart is shown three records of the first 10% dextrose infusion. The first two are crossed out, with the third being the dose which was administered.
The judge asks to clarify that the only difference between the three records is the rate of infusion for the 10% dextrose bag. Dr Bhowmik confirms that is correct.
That concludes Dr Bhowmik's evidence.
Neonatal Practitioner Amy Davies
See also: INQ0017825 – Witness Statement of Amy Davies, dated 10/04/2024
The court is now hearing evidence from Amy Davies, a neonatal practitioner who was employed in the neonatal unit at the Countess of Chester Hospital in April 2016. At the time, she was in Band 6.She says she does not have any independent recollection of Child L.
From her notes, she was on the day shift on April 8, 2016, as shift leader. Lucy Letby was the designated nurse for Child L on the 8th, and Ms Davies confirms she assisted in the care.
She is asked if there was a specific pathway for babies with low blood sugar. Ms Davies confirms there was, and would involve giving milk before giving IV fluids with glucose, but each case differed.
In this case, a discussion would have taken place with the doctor, Ms Davies confirms. She said it was a decision which would not put the baby at risk, but was an alternative pathway.
Asked if she had any concerns about that pathway, Ms Davies replies: "No, no concerns."
The blood gas records show glucose levels for Child L on April 8 at 1.9 (10.58am) and 2.5 (12.14pm). The readings go above 2.5 in subsequent blood gas records for April 8, which only test for glucose levels.
She confirms she would have checked the infusion bag containing 10% dextrose with Lucy Letby, making sure it was in date, going to the right baby, and signing it. The infusion is noted as starting at noon on April 8.
Ms Davies says the pre-made dextrose concentrations available for infusion bags are 5% and 10%.
Ms Davies says the bags would be changed, regardless, every 48 hours.
Ms Davies is asked if she, at any point, administered Child L with insulin. She replies she did not, and is not aware of anyone doing so.
She says the circumstances for doing so would be two consecutive blood sugar readings of 12 or above, if a baby was hyperglycaemic.
Cross Examination
Mr Myers, for Letby's defence, asks if Ms Davies was one of the nurses who transferred Child L and Child M to the neonatal unit.
Ms Davies confirms she would have been the designated nurse for Child M at that time.
Ms Davies is asked about the hypoglycaemic pathway. She says she is familiar with it, but keeps checking as policies regularly update. She confirms one was in place at the time.
Mr Myers says the policy was milk first, then IV fluids, in normal circumstances. He says circumstances mean a doctor might change that and go to IV fluids.
Ms Davies agrees.
Mr Myers says there are three types of nutrition bag available - start-up bags for the baby's first couple of bags, maintenance bags, and specifically prescribed TPN bags which would have a baby's name on it. Ms Davies agrees.
She tells the court the bag for Child L wouldn't have been referred to as a start-up bag, but would have been a standard 10% dextrose bag, as prescribed, to be infused.
That completes Ms Davies's evidence.
Dr Anthony Ukoh
See also: INQ0106972 – Witness Statement of Dr Anthony Ukoh, dated 20/07/2024.
Dr Anthony Ukoh is called to give evidence.He says his recollection was that Child L and Child M were born premature, not extremely so, and for Child L, he did not have any 'red flags' as a baby who would become unwell.
Dr Ukoh's notes for Child L from April 9, 2016, at 10.20am, are shown to the court.
He noted the baby was breathing well, and Child L was on an extra 10% dextrose dose as the blood sugars were running at a "relatively low level for his age", but was "not unusual" for premature babies.
There were no 'red flags' from the observations.
The plan was 'as per hypoglycaemic protocol', to increase the infusion of 10% dextrose administration, "to make up for the low blood sugars", and to repeat blood sugar checks.
Dr Ukoh confirms a hypo screen test result, taken at noon on April 9, which is handwritten, is in his writing.
He says it is not a complete hypo screen results sheet, and said that would have been done in response, and at the time of, a low blood sugar reading.
Some of the results would have required sending away for analysis.
He says the test results would have been received by the lab at 6.26pm.
Cross Examination
Mr Myers, for Letby's defence, asks to clarify Dr Ukoh's explanations for the way some of the results are presented.
The judge asks for the hypoglycaemic blood test, if there was just one blood sample taken from Child L for the various tests carried out.
Dr Ukoh agrees that was the case, and that some of the results would not come back straight away.
Dr A [Thirlwall: Dr U]
See also: Dr U's oral testimony at the Thirlwall Inquiry
Taken from Daily Mail as more detailedA nurse accused of murdering seven babies and attempting to kill a further ten broke down in tears today as a paediatric consultant gave evidence.
Lucy Letby, 33, was visibly upset and even appeared to try to leave the courtroom as she stood in the dock and walked swiftly to the door leading to the cells.
A female security officer approached her for a hushed conversation.
Letby took a few moments to compose herself before returning to the seat she has occupied throughout her 16-week trial at Manchester Crown Court.
The outburst was triggered by the paediatrician, who cannot be named for legal reasons, beginning to give evidence from behind a privacy screen, blocking his view of the dock.
It prompted the trial judge, Mr Justice Goss, to ask a defence solicitor to 'just see what the problem is'.
A lawyer walked the few feet to the dock and spoke briefly to Letby through the glass screen, and moments later the defendant's barrister, Ben Myers KC, had his own conversation with her.
Letby was still wiping tears from her eyes, this time with tissues from a box beside her, as the proceedings resumed.
The consultant was asked for a second time to confirm his name and occupation. His evidence lasted only a few minutes as he took Philip Astbury, prosecuting, through some medical notes relating to Baby L, one of a set of twins whom Letby is alleged to have injected with insulin.
The consultant told the court the child's blood sugar levels were decreasing during the night shift and were 'lower than what I would have wanted'.
When asked why it was necessary to stop the levels falling, he said: 'Because low blood glucose levels in a baby can cause seizures.
'It's damaging to a baby. If it falls to a much lower level, then it can cause liver damage and brain injury.'
Mr Myers rose to say that he had no questions to ask in cross-examination.
Dr John Gibbs
See also:
INQ0008978 - Pages 4 & 5 of letter from Dr John Gibbs to Mother & Father C re Child C's death, dated 24/09/2015
INQ0001993 – Page 14 of Witness statement of Dr John Michael Gibbs, for the trial of R v Letby, dated 20/11/2017
Dr John Gibbs' oral testimony at the Thirlwall Inquiry
Later Dr John Gibbs, the lead paediatrician on the unit at the time, told the court blood tests carried out on Baby L confirmed he had been 'given insulin that he should not have received'.
He added: 'I was not thinking at the time that someone might have administered insulin. The results showed that, but unfortunately the junior doctors who read them didn't realise the significance'.
Dr Anna Milan
See also: Dr Anna Milan's oral testimony at the Thirlwall Inquiry
From Dan O’Donohue Twitter (20/02/2023)Anna Milan, a clinical biochemist, is giving evidence about a blood sample analysis that was carried out for Child L. The analysis was to test for insulin
Court is being shown blood analysis results for
Child L (they were collected on 9 April 2016). Ms Milan said the 'only way you get a pattern like that is if insulin has been given to a patient'
Cross Examination
Ben Myers KC, defending, is now questing Dr Milan on the process for analysing blood - from ward to lab. She says 'ideally' blood will be taken and cooled within 30minutes to preserve it. Mr Myers asks if blood is left for hours, will it cause issues - 'it can do yes'
Mr Myers asks if a sample hasn't been handled correctly, will it effect the relatability of the findings - and specifically in this case. Dr Milan says it can effect findings, but it 'wouldn't create insulin in this sample'
Dr Milan repeats, that the only explanation for the readings in this sample is external administration
Dr Gwen Wark
From Dan O’Donohue Twitter (20/02/2023)Dr Gwen Wark is now in the witness box. She is the director of the Guildford RSCH Peptide Hormone Laboratory. Her evidence again focuses on the blood analysis of Child L
Dr Wark's evidence relates to the veracity of the blood test results. She confirms Child L's reports met all required standards
Medical Expert Evidence
Professor Peter Hindmarsh
A medical expert told Manchester Crown Court that the youngster, Child L, suffered a hypoglycaemic episode which lasted from the morning of April 9, 2016 to the middle of the afternoon on April 11.Peter Hindmarsh, professor of paediatric endocrinology at University College London, said the results of a blood sample taken some time on the afternoon of April 9 meant he was “quite certain” that non-natural insulin was present in his system.
Nick Johnson KC, prosecuting, said: “So somebody gave insulin to?”
Prof Hindmarsh replied: “Yes, I agree with that statement and I think we should add that it was not prescribed insulin.”
Giving evidence on Friday, he considered the most likely method of administration was intravenously into a bag of dextrose, a sugar supplement, which was connected to Child L’s drip.
Prof Hindmarsh said the volume of insulin required would be “quite small” and would not be noticeable in the bag or from a routine stock check.
He added: “Once in the bag it’s – in a sense – sealed off from you being able to detect it by smell.”
Jurors heard the dextrose concentration was increased as medics tried to bring Child L’s blood sugar levels up – which necessitated a change of bag – and the rate of infusion was also stepped up.
Prof Hindmarsh said despite that there was “not really much change in the glucose measurements which would imply there was ongoing insulin present and ongoing insulin action”.
He told the court that insulin could “potentially” have been added to at least three dextrose bags if the giving sets were also changed.
Prof Hindmarsh also raised the possibility that if the giving set remained the same then insulin could stick to its plastic, come off and then release into the bag.
Cross Examination
He agreed with Ben Myers KC, defending, that “sticky insulin” would eventually run out.
Mr Myers asked: “It is the case that sticky insulin could be operative over a similar period?”
Prof Hindmarsh replied: “I don’t think anyone has done this sort of study to be honest. I think the answer is I don’t know.”
He told Mr Myers the “relatively steady” blood sugar levels did not seem to be influenced by the increased infusion rates.
Mr Myers asked: “Would that be more consistent with it being added to the bag as you go on, rather than the sticky insulin?”
Prof Hindmarsh replied: “Yes.”
Police Interviews Summary
When later interviewed by Cheshire Police following her arrest Letby denied deliberately administering insulin to Child L, who cannot be identified for legal reasons.She said to her knowledge neither she nor a nursing colleague had accidentally administered the substance, which had not been prescribed.
Letby added she could not believe such a mistake would have been made.
When suggested by detectives it was a deliberate act of sabotage, the defendant replied: “That was not done by me.”
Asked if she had any explanation for the presence of insulin in Child L’s circulation she said it “must have been in one of the bags or fluids he was receiving”.